
Effective patient communication in dentistry
Why words alone struggle to close the case
A patient sits in the chair after a longer-than-usual exam. The dentist has found three things that need attention - one urgent, two within the next year. The explanation is careful, clear, unrushed. And by the time the patient walks out, half of what was said is already gone.
This isn’t a failure of the dentist’s communication. It’s the shape of the moment itself. Nobody absorbs a multi-thousand-euro clinical decision in fifteen minutes of one-way explanation, especially when the room smells faintly of disinfectant and the patient is still tasting fluoride. Patient communication in dentistry has to survive the trip from the chair to the moment of decision, and most of it doesn’t.
Patient communication isn’t a soft skill. It’s the thing that decides whether a diagnosis becomes treatment, whether the patient becomes loyal, and whether clinical work translates into the outcome the dentist proposed. The hardest part is rarely what happens in the room. It’s everything that happens after.
Where most clinics lose the patient
Healthcare research is consistent about one thing: communication failure has a measurable cost. One large analysis of malpractice claims attributed communication breakdowns to roughly $1.7 billion in damages, according to a HIPAA Journal review of CRICO Strategies research. Dentistry rarely sits at that severity end of the spectrum, but the same dynamic plays out at the business end of the chair: case acceptance for the majority of dental practices is far below what the clinical quality of their work would suggest.
The pattern is almost always the same. The clinical work is sound. The proposal is fair. The conversation in the chair is competent. What breaks is the medium through which the plan is communicated to the patient. And in most clinics, that medium is a generic, text-heavy document handed over at the front desk - one that reads more like an invoice than a proposal, full of clinical jargon and billing codes, with no visual structure to support what was just explained.
The treatment plan is the moment of truth
In traditional dental software, the patient-facing document is an administrative afterthought, the last step in a billing process rather than a designed piece of communication. The output is a sheet that overwhelms the patient instead of informing them. It creates anxiety at the precise moment a financially significant decision is being asked for. It erodes the trust the dentist has spent thirty minutes building.
It also forces the clinic to do the same work twice. Dentists and treatment coordinators end up manually deciphering their own plans for patients. Presenting multiple options side by side - which is a normal clinical reality, not an edge case - becomes nearly impossible to do live in a high-pressure consultation, with a sheet of paper that wasn’t designed to compare them.
The downstream effect is predictable. Indecision becomes the default. Case acceptance drops, disproportionately for the high-value cases the clinic depends on. And the practice itself, regardless of how thoughtful its clinical care is, ends up being represented to the patient by its weakest artifact.
Patients decide best when the plan looks like it was made for them.
What visualization does to patient understanding
The research on visual aids in patient communication is unusually consistent.
A 2024 systematic review of visual aids for surgical patient education found that most of the studies it covered showed statistically significant improvements in patient comprehension when illustrated materials were used in place of standard verbal or text instructions. A separate patient-education review cites adherence research where adding visual aids drove a 25% increase in patients actually following the plan.
This isn’t decoration. The visual is doing real cognitive work. It anchors what the dentist said. It gives the patient a structure to think about the decision instead of a memory they’re trying not to lose. It collapses the distance between a technical diagnosis and a non-technical understanding.
In dentistry specifically, a randomized trial in pediatric practice found that using intraoral scans as a visual aid measurably improved how dental findings were communicated. The mechanism is the same across studies. See the thing, understand the thing, decide on the thing.
What an effective treatment plan looks like
Comparing the documents produced by clinics with consistently high acceptance against the documents produced by clinics struggling with it, a few patterns separate them:
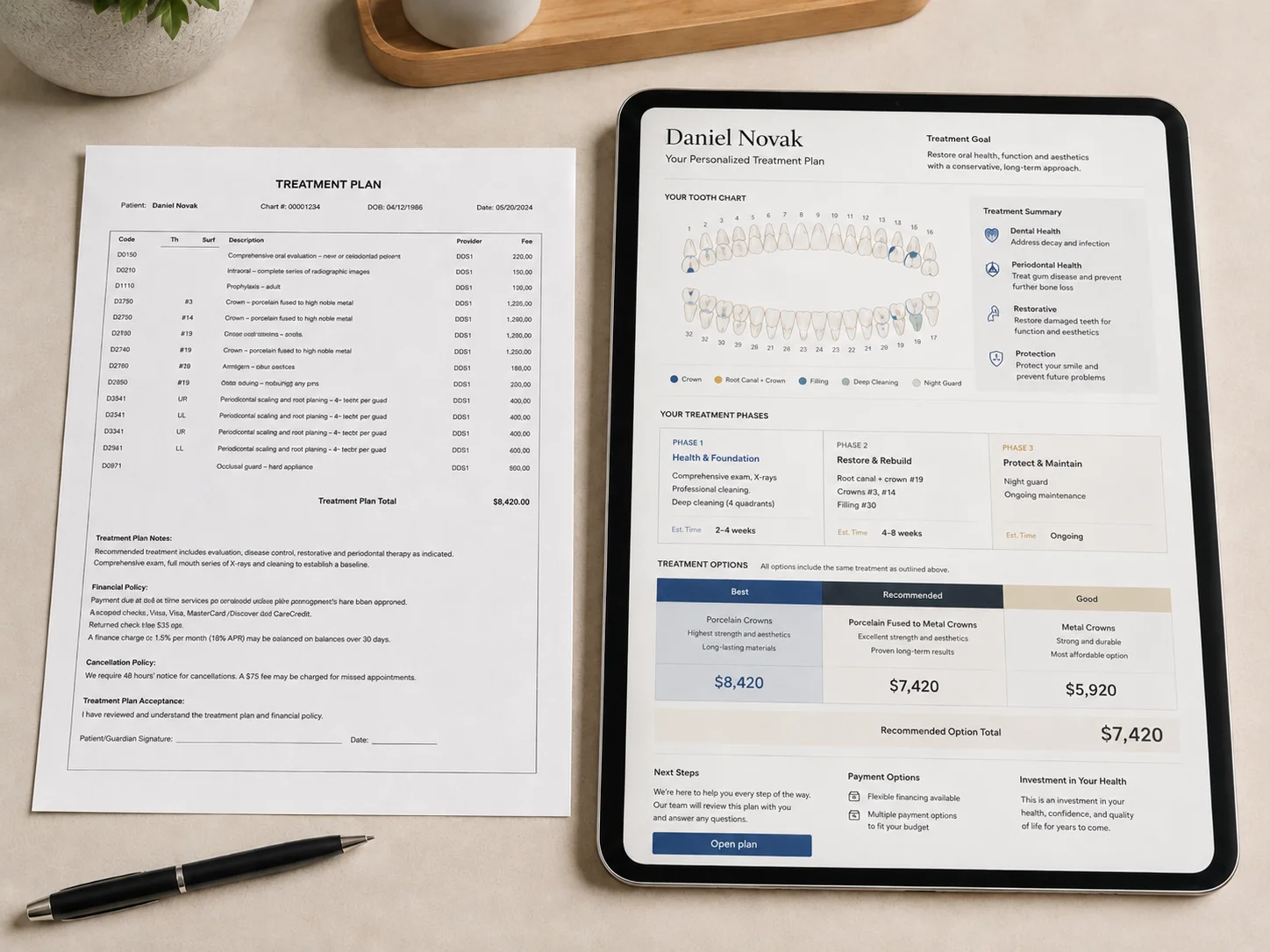
- The document is visual, not textual. A tooth chart, an annotated X-ray, an intraoral scan inside the plan itself. The patient sees what the dentist saw, not a paragraph describing it.
- Phasing is laid out as a sequence. “First this, then this, then this.” Phased layouts also signal that the plan is thoughtful, not opportunistic.
- Options are presented side by side. When a plan presents an implant and a bridge as comparable choices, the patient feels informed. When it presents one as the only path, the patient leaves and reads about the other one online.
- Pricing is structured and transparent. Not necessarily lower, clearer. Patients accept high-ticket treatment when they understand what they are paying for.
- The document is branded. It reflects the clinic, not the software. A high-quality practice represented by a low-quality document is a contradiction patients notice.
- The document is interactive, not static. It can be sent digitally, opened on a phone, expanded, commented on, and accepted inside the document itself. Revisions go out the same way without forcing anyone to reprint or re-explain.
A treatment plan built this way is doing more than informing. It is selling the value of the treatment. The same clinical content, in a different vehicle, behaves like a different proposal.
What changes when the plan is digital and interactive
A static PDF disappears into an inbox. A digital plan behaves like a small piece of software: patients can expand sections, compare options, see financing scenarios, comment, accept or reject inside the plan itself. The interactivity is part of the communication, not a separate channel.
It also gives the clinic something a paper plan cannot: visibility into what happens after the consultation. Whether the plan was opened. Which option the patient spent the most time on. Whether questions are coming in. Whether a follow-up is timely or already overdue. That visibility turns ad hoc follow-up into a process the clinic can actually run, and lets the treatment coordinator reach the patient while they are still engaged, with context, instead of with a sticky note two weeks later.
The interactive document doesn’t replace the conversation in the chair. It carries forward what was said in a form the patient can use, and it gives the clinic something to react to instead of waiting.
Where this leaves the clinic
The clinics that consistently sit at the high end of case acceptance are not the ones with the smoothest verbal pitch. They are the ones whose patients are handed a plan that does the work of communication on its own - visual, branded, structured, comparable, interactive. They invest in the document because the document is the thing the patient is actually using to make the decision.
If acceptance is lagging the clinical quality of the work, the question to look at first is not how well the dentist is explaining things in the room. It is what the patient sees when they look at the plan. If that artifact looks like an invoice, that is where the consultation is breaking down.
Plandentic is built around that artifact. The clinical plan becomes a visual, branded, interactive document the clinic shares digitally with the patient, with phased treatment, side-by-side options, structured pricing, and a portal the patient can engage with directly. The clinic also gets visibility into how the plan is being used: which plans are sitting, which patients are active, where to follow up next. The conversation in the chair remains the clinic’s. The document is what carries the value forward.

